Given the heightened concerns related to the spread of COVID-19, we ask that you please fax/and or email your completed Authorization Forms.
Clinic Record Pick-up Announcement
Fax Number: 570-273-0989
Email: ROI@berwickhospitalcenter.com
Instructions for the form are as followed:
- If the records are strictly for the patient, please fill out the section titled Patient.
- If you would like a secure e-mail, please provide your e-mail address on the form. Following your submission please send an e-mail to: ROI@berwickhospitalcenter.com with; patients Name, requestors name and date of birth. This is part of our two step verification to ensure the protection of your health information.
- If someone else is picking up the records on behalf of the patient, please have their information filled out in the section titled Other Individual/Company.
- If the records are for your doctor, please fill out the doctor’s information where it states Other Individual/Company.
- If records are going to more than one person, please complete one form per recipient (i.e. if records are going to the patient AND a doctor, please complete one form for the patient and one form for the doctor; a total of two forms must be completed).
- Please include the date of service and/or tests being requested.
Personal Representative
If the patient is unable to sign the authorization, copies of one of the following documents would have to be provided:
- Healthcare Proxy OR
- Medical Power of Attorney OR
- Guardianship Letter
Deceased Patients
If the patient is deceased a copy of the death certificate must be provided along with one of the following documents;
- Letter of Administration OR
- Letters Testamentary OR
- Distributee Affidavit
Minors
Parents of minors (under 18 years of age), next of kin or legally appointed guardians, may obtain a copy of a minor’s record.
Exception:
If a minor from the ages of 12 -17 was treated for sexually transmitted disease, birth control treatment, drug/alcohol abuse treatment, HIV or mental illness, the records can only be released upon the minor’s authorization.
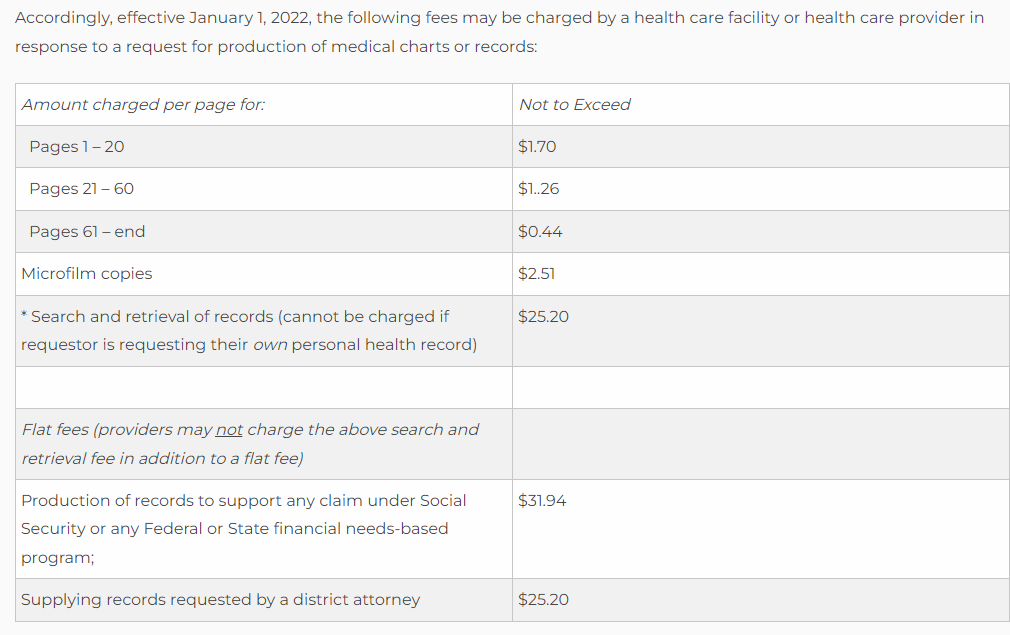
New York State Public Health Law allows Berwick Hospital Center to charge a reasonable fee to recover the costs of copying, mailing and supplies used to fulfill your request. Patients will receive a pre-bill or a payment notice with their records. However. there is no fee if the record is being released to a doctor or healthcare provider for continuity of care.
Once the authorization is completed you can mail. email or fax the release form to the contact information below.
Authorizations are processed within 7 to 10 business days of receipt.
Any questions or concerns please feel free to reach out.
ROI
Department of Medical Records Berwick Hospital Center
A member of the BHC Health System
701 East 16th Street, Berwick, PA 18603 Office: (570) 759-5000
Fax: (570) 273-0989
Please provide a copy of your photo identification.